
Your gift is 100% tax deductible.
Your Breast Pathology Report: Breast Cancer
Learn about some of the medical terms in a pathology report that shows breast cancer.
On this page
- Types of breast biopsies
- Breast anatomy
- What is a carcinoma or adenocarcinoma?
- Types of invasive carcinomas
- Vascular, lymphovascular, or angiolymphatic invasion
- Breast cancer grade
- Estrogen receptor (ER) and progesterone receptor (PR) status
- HER2 (HER2/neu) status
- Stage (extent) of breast cancer
- Lymph node tests
- Other terms that might be on a pathology report
- Other lab tests that might be done
Types of breast biopsies
A biopsy is a procedure that removes small pieces of tissue so they can be examined under a microscope or tested. A breast biopsy can be done by:
- Needle biopsy, where a hollow needle is used to remove samples from an abnormal area in your breast.
- Incisional biopsy, a type of surgical biopsy in which only part of an abnormal area is removed.
- Excisional biopsy, a type of surgical biopsy that removes the entire abnormal area, often with some of the surrounding normal tissue. It is much like a lumpectomy, a type of breast-conserving surgery.
After biopsy samples are collected from your breast, they are studied by a pathologist, a doctor who specializes in diagnosing and classifying disease. After testing the samples, the pathologist creates a pathology report on what was found. Your doctors can use this report to help manage your care.
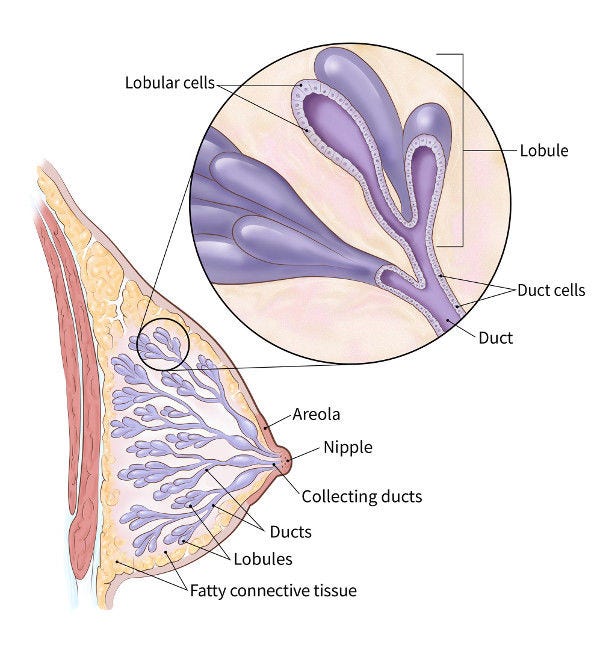
Breast anatomy
The normal breast contains milk ducts (tiny tubes) that end in groups of sacs called lobules (where milk is made). Ducts, lobules, and many other organs in the body are lined by a layer of tissue called epithelium.
What is a carcinoma or adenocarcinoma?
Carcinoma is a term used to describe a cancer that begins in the lining layer (epithelium). Nearly all breast cancers are carcinomas. Most of these are a type of carcinoma that starts in glandular tissue, which is called an adenocarcinoma.
In-situ carcinoma
In-situ carcinoma, also known as carcinoma in situ or CIS, means that abnormal cells are growing in the lining (epithelium) of the ducts or lobules but they aren’t invading into deeper tissue layers.
Infiltrating or invasive carcinoma
If the carcinoma cells have grown (invaded) deeper than the epithelium, this is called an invasive or infiltrating carcinoma. This is a true cancer, meaning that the tumor cells can grow outside the breast or spread (metastasize) to other parts of the body.
Types of invasive carcinomas
The main types of invasive breast carcinomas are:
- Invasive ductal carcinoma (IDC) or invasive mammary carcinoma of no special type
- Invasive lobular carcinoma (ILC)
- Mixed ductal and lobular carcinoma or carcinoma with ductal and lobular features
Invasive ductal carcinoma is the most common type of breast cancer.
In general, these cancers are treated similarly, although there might be some slight differences. These differences might become more pronounced in the future, as some drugs now being studied might be more useful for invasive lobular cancers.
Types of IDC
Different types of IDC can be identified under the microscope:
- Tubular, mucinous, and cribriform carcinomas are types of well-differentiated IDC that tend to have a better prognosis (outlook) than the more common type of IDC (invasive mammary carcinoma of no special type).
- Micropapillary carcinoma tends to grow and spread more quickly.
In some situations, different treatments might be recommended for these types of breast cancer.
Since some breast cancers are made up of more than 1 type, the entire tumor must be removed by lumpectomy or mastectomy in order to know what types your tumor contains.
Vascular, lymphovascular, or angiolymphatic invasion
If cancer cells are seen in small blood vessels or lymph vessels (lymphatics) within the tumor, it is called vascular, angiolymphatic, or lymphovascular invasion.
When cancer is growing in these vessels, there is an increased risk that it has spread outside the breast.
Even if this type of invasion is there, it doesn’t always mean that your cancer has spread.
Breast cancer grade
Certain features of the cancer can help predict how likely it is to grow and spread. These features include:
- Gland formation, which describes how closely the arrangement of cells looks like normal milk glands.
- Nuclear grade, which describes how much the nuclei of the cells (where the DNA is) look like those of normal breast cells.
- Mitotic count, which describes how many of the cancer cells are in the process of dividing to make new cells.
Taken together, these features determine the grade of the cancer. The grade can be described in different ways.
Differentiation
The cancer grade is sometimes described using differentiation, or how closely the cancer cells and their arrangements look like those of normal, mature breast cells.
- Well-differentiated carcinomas have relatively normal-looking cells that are growing in patterns that are close to normal. These cancers tend to grow and spread slowly and to have a better prognosis.
- Moderately differentiated carcinomas have cells and growth patterns that look a little more abnormal.
- Poorly differentiated carcinomas lack normal features. They tend to grow and spread faster.
Histologic grade
The cancer grade can also be described using a histologic grade, also called the Nottingham grade, or Elston grade. The 3 features above are each given a score from 1 to 3, and their sum is used to assign the grade.
Sum |
Grade |
Differentiation |
3 to 5 |
1 |
Well-differentiated |
6 or 7 |
2 |
Moderately differentiated |
8 or 9 |
3 |
Poorly differentiated |
Estrogen receptor (ER) and progesterone receptor (PR) status
If breast cancer is found on the biopsy, the cells will be tested for hormone receptors.
Receptors are proteins on cells that can attach to certain substances, such as hormones that circulate in the blood and breast tissue. Normal breast cells and some breast cancer cells have receptors that attach to the hormones estrogen and progesterone. These hormones often fuel the growth of the cancer cells.

On your pathology report
Cancer cells might contain neither, one, or both of these receptors.
- ER-positive or ER+ means it has estrogen receptors (ER).
- PR-positive or PR+ means it has progesterone receptors (PR).
Results for ER and PR are reported separately, and they might be reported in different ways:
- Negative, weakly positive, or positive
- Percent positive
- Percent positive and whether the staining is weak, moderate, or strong
Cancers that are ER-positive or PR-positive (or both) are considered to be hormone receptor-positive (HR+). HR+ cancers tend to have a better prognosis and are much more likely to respond to hormone therapy than cancers without these receptors. Ask your doctor how these results might affect your treatment.
HER2 (HER2/neu) status
HER2-positive breast cancers have too many copies of the HER2 gene, which instructs the cells to make too much of the HER2 or HER2/neu protein. This helps them grow.
These cancers tend to grow and spread more quickly than other breast cancers, but they are also more likely to respond to drugs that target the HER2 protein.
Tests for HER2
Testing for HER2 can be done in several ways. Immunohistochemistry is often used first. This might be followed by the FISH test to further classify the tumor type.
In this test, special antibodies that will stick to the HER2 protein are applied to the sample, which cause cells to change color if they have higher levels of HER2 protein. This color change can be seen under a microscope. The test results are reported as 0, 0+, 1+, 2+, or 3+.
This test uses fluorescent pieces of DNA that specifically stick to copies of the HER2 gene in cells, which can then be counted under a special microscope.
While the FISH test is more accurate than IHC, it is more expensive, and it takes longer to get the results.
CISH is a newer test that works similarly to FISH, by using small DNA probes to count the number of HER2 genes in breast cancer cells. This test looks for color changes (not fluorescence) and doesn't require a special microscope, which might make it less expensive than FISH. It is not used as much as IHC and FISH.
Possible test results
After testing for HER2 status, several different results might appear on a pathology report. Ask your doctor how the results of these tests might affect your treatment.
In this case, the IHC result is 0 with no membrane staining. These cancers do not respond to treatment with drugs that target HER2.
In this case, the IHC result is 0 with membrane staining (HER2+ staining in more than 0% but no more than 10% of tumor cells). These cancers might respond to drugs called antibody-drug conjugates.
In this case:
- The IHC is 1+, OR
- The IHC is 2+ but FISH is negative
These cancers might respond to certain drugs called antibody-drug conjugates.
In this case:
- The IHC is 2+ and the FISH is positive, OR
- The IHC is 3+
These cancers often respond to drugs that target HER2.
Stage (extent) of breast cancer
The stage of a breast cancer is based on the size of the tumor and if the cancer has spread, as well as certain other characteristics such as the tumor grade.
The staging system most often used for breast cancer is the American Joint Committee on Cancer (AJCC) TNM system, which relies mainly on 3 key pieces of information:
- The T category is based on the size of the tumor and whether it has reached the skin over the breast or the chest wall under the breast.
- The N category indicates if the cancer has spread to lymph nodes near the breast and, if so, how many lymph nodes are affected.
- The M category stands for metastasis (spread to distant parts of the body). It is usually based on the results of exams and imaging tests, so it’s not normally part of a pathology report from a breast biopsy or surgery.
Numbers or letters after T, N, and M provide more details about each of these factors. Higher numbers mean the cancer is more advanced.
Once the T, N, and M categories, the tumor grade, estrogen receptor (ER) and progesterone receptor (PR) status, and HER2 status have been determined, this information is combined to give the cancer an overall stage. Non-invasive cancer (ductal carcinoma in situ, or DCIS) is listed as stage 0.
For more information, see Stages of Breast Cancer and Cancer Staging. Talk with your doctor about the stage of your cancer and what it might mean for you.
Lymph node tests
If breast cancer spreads, it often goes to the lymph nodes under the arm (axillary lymph nodes) first. Lymph node spread affects the stage of the cancer as well as a person’s prognosis.
The sentinel lymph nodes are the first lymph nodes to which a tumor drains. They are most likely to contain cancer cells if breast cancer starts to spread.
Sometimes, a procedure known as a sentinel lymph node biopsy (SLNB) is done to identify the sentinel lymph nodes and check them for cancer.
If there is no cancer in the sentinel nodes, it's very unlikely that the cancer has spread to other lymph nodes, so no further lymph node surgery is needed.
If a sentinel lymph node contains cancer, you might need further treatment, such as surgery to remove more underarm lymph nodes or radiation therapy to the underarm region. You should discuss this with your doctor.
If your pathology report mentions isolated tumor cells, that means there are only small numbers of cancer cells in the lymph node. Isolated tumor cells do not affect your stage or change your treatment.
pN0(i+) means that isolated tumor cells were found in a lymph node using routine or special stains.
pN0(mol+) means that isolated tumor cells could only be detected in a lymph node by using very sensitive molecular tests.
Micrometastases are larger groups of cancer cells in the lymph node than isolated tumor cells, but these groups are still smaller than regular cancer deposits. If micrometastases are present, the N category is listed as pN1mi. This can affect the stage and treatment of your cancer.
Talk to your doctor about what these findings might mean for you.
Other terms that might be on a pathology report
You might see other medical terms on your pathology report. Many of these are benign changes. Usually, they are not important when seen on a biopsy where there is breast cancer.
Benign (noncancerous) changes
Benign changes that might be noted on a pathology report include:
- Usual ductal hyperplasia (UDH)
- Adenosis or sclerosing adenosis
- Radial scar or complex sclerosing lesion
- Papilloma or papillomatosis
- Apocrine metaplasia
- Columnar cell change
- Collagenous spherulosis
- Duct ectasia
- Fibrocystic changes or cysts
- Flat epithelial atypia (FEA)
- Columnar alteration with prominent apical snouts and secretions (CAPSS)
These are not important when seen on a biopsy result that also shows invasive breast cancer.
Atypical or precancer changes
Types of atypical or precancer breast changes include:
- Atypical ductal hyperplasia (ADH)
- Atypical lobular hyperplasia (ALH)
- Ductal carcinoma in situ (DCIS) or intraductal carcinoma
- Lobular carcinoma in situ (LCIS) or in-situ lobular carcinoma
These might need to be removed completely as a part of treatment.
If found on an excisional biopsy, at or near a margin, more breast tissue might need to be removed, even if all of the invasive cancer was taken out.
If they are found in a needle biopsy that also shows invasive cancer, they typically are not important.
For more on these conditions, see:
Microcalcifications or calcifications
Microcalcifications or calcifications are small calcium deposits that can be found in both noncancerous and cancerous breast lesions. They can be seen both on mammograms and under a microscope.
Because certain calcifications can be found in areas containing cancer, their presence on a mammogram might lead to a biopsy of the area. Once the biopsy is done, the pathologist looks at the removed tissue to be sure that it contains calcifications. If the calcifications are there, the doctor knows that the biopsy sampled the correct area (the abnormal area on the mammogram).
Margins or ink
When an entire tumor and some surrounding normal breast tissue is removed, the margins (edges) of the specimen are coated with ink. This helps the pathologist tell whether the abnormal area was removed completely when looking at it under a microscope. If cancer cells are touching the ink, called positive margins, it can mean that some cancer cells were left behind and more surgery or other treatments might be needed. Sometimes, though, the surgeon has already removed more tissue during surgery to help make sure that this isn’t needed.
Sometimes, all the invasive cancer is removed, but there might be precancer or another serious condition at or near the margin, such as ductal carcinoma in situ (DCIS).
If your pathology report shows positive margins, your doctor will talk to you about what treatment is best.
Other lab tests that might be done
Other lab tests might be done to get more information about your breast biopsy.
E-cadherin is a test that might be used to help determine if the tumor is ductal or lobular. The cells in invasive lobular carcinomas are often negative for E-cadherin. If your report doesn’t mention E-cadherin, it means that this test wasn’t needed to tell what type of cancer you have.
D2-40 and CD34 are special tests that might be used to help identify the different types of vascular invasion in a tumor. These tests are not always needed.
Ki-67 is a way to measure how fast the cancer cells are growing and dividing. Higher values for Ki-67 (typically over 30%) mean that many cells are dividing, so the cancer is likely to grow and spread more quickly.
Other tests that might be used to help diagnose invasive breast cancer or to identify cancer in lymph nodes include:
- High molecular weight cytokeratin (HMWCK)
- CK903, also known as 34betaE12
- CK5/6
- p63
- Muscle specific actin
- Smooth muscle myosin heavy chain
- Calponin
- Keratin
Not all biopsies need these tests. If these tests appear on your pathology report, ask your health care provider what the results mean for you.
Your breast cancer cells might be tested for other gene or protein changes, especially if your cancer is more advanced. Tests for these changes can show if certain types of medicines such as targeted therapy, hormone therapy, or immunotherapy drugs might be helpful in treating your cancer. For example, tests might be done to look for:
- BRCA1 and BRCA2 gene changes
- PIK3CA, AKT1, and PTEN gene changes
- ESR1 gene mutations
- NTRK gene changes
- PDL-1 protein levels
- Microsatellite instability (MSI) and mismatch repair (MMR) gene changes
- Tumor mutational burden (TMB)
For more on these tests, see Other Breast Cancer Gene, Protein, and Blood Tests.
Gene expression profiling, also called genomic testing, can look at the activity of many different genes at once. Examples of these tests include:
- Oncotype DX
- MammaPrint
- Prosigna
- EndoPredict
- Breast Cancer Index (BCI)
These tests might be done in some situations to help predict the prognosis for people with breast cancer or to determine if certain treatments are likely to be helpful, but not everyone needs these tests.
If your doctor orders this test, ask your doctor to explain what the results mean. The results don’t affect your diagnosis, although they might affect your treatment options.
- Written by
- References

Developed by the American Cancer Society medical and editorial content team with medical review and contribution by the American Society of Clinical Oncology (ASCO).
Bleiweiss IJ. Pathology of breast cancer. UpToDate. 2026. Accessed at https://www.uptodate.com/contents/pathology-of-breast-cancer on March 18, 2026.
Joe BN. Clinical features, diagnosis, and staging of newly diagnosed breast cancer. UpToDate. 2026. Accessed at https://www.uptodate.com/contents/clinical-features-diagnosis-and-staging-of-newly-diagnosed-breast-cancer on March 23, 2026.
National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology: Breast Cancer. Version 3.2026. Accessed at https://www.nccn.org on May 21, 2026.
Last Revised: May 21, 2026
American Cancer Society medical information is copyrighted material. For reprint requests, please see our Content Usage Policy.
American Cancer Society Emails
Sign up to stay up-to-date with news, valuable information, and ways to get involved with the American Cancer Society.

