
Your gift is 100% tax deductible.
Your Colon or Rectal Pathology Report: Polyps (Including Serrated Adenomas)
Biopsy samples collected from your colon or rectum are studied by a doctor with special training, called a pathologist. After testing the samples, the pathologist creates a report on what was found. Your doctor can then use this report to help manage your care.
The information here is meant to help you understand some of the medical terms you might see in your pathology report after your colon or rectum is biopsied.
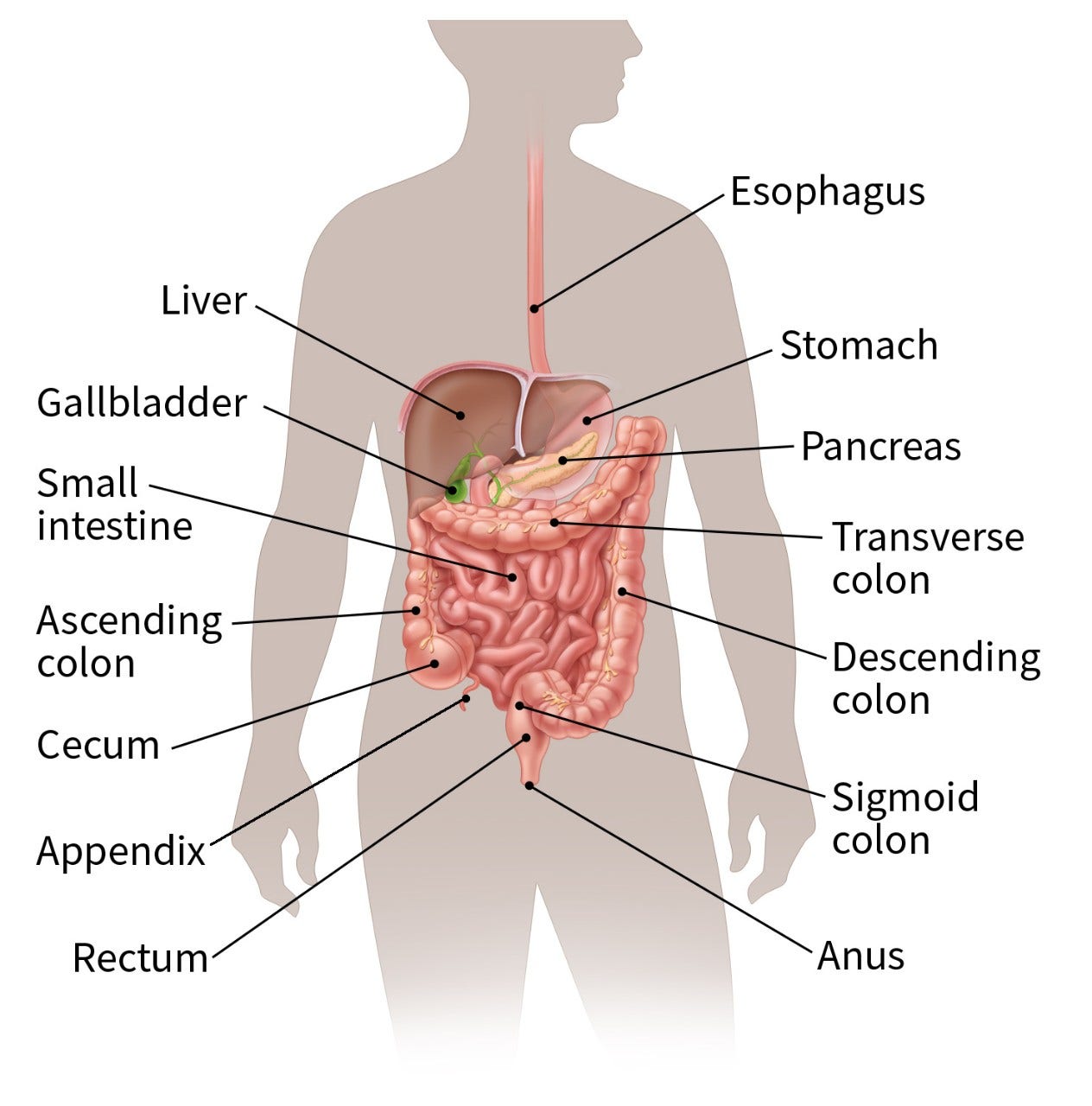
Parts of the colon and rectum
The colon and rectum make up the large intestine (or large bowel), which is part of the digestive system. The cecum is the beginning of the colon, where the small intestine empties into the large intestine. The ascending colon, transverse colon, descending colon, and sigmoid colon are the parts of the colon after the cecum. The colon ends at the rectum, where waste (stool) is stored until it leaves the body through the anus.
Colon or rectal polyps
A polyp is a projection (growth) from the inner lining into the lumen (hollow center) of the colon or rectum.
There are different types of polyps, which look different when seen with a microscope. Most polyps are benign (non-cancerous) growths, but cancer can start in some types of polyps.
For example, hyperplastic polyps are typically benign (not cancer or pre-cancer) and are not a cause for concern. But the different types of adenomatous polyps (adenomas), which are discussed below, are more of a concern because they might turn into cancer. These polyps can be thought of as pre-cancers, which is why it is important to remove them.
Types of adenomas
An adenoma (adenomatous polyp) is a type of polyp made up of tissue that looks a lot like the normal inner lining of your colon or rectum, although it is different in some important ways when looked at under a microscope.
There are different types of adenomas, which are often described based on their growth patterns.
Tubular, tubulovillous, and villous adenomas
Adenomas can have 2 major growth patterns: tubular and villous. Many adenomas have a mixture of both growth patterns, so they are called tubulovillous adenomas.
Most small adenomas (less than ½ inch) have a tubular growth pattern. Larger adenomas are more likely to have a villous growth pattern.
Larger adenomas and adenomas with a villous growth pattern are more likely to have cancer cells in them.
The growth pattern in a polyp can be important, because it can help determine when you will need your next colonoscopy. But when a polyp is biopsied, the most important things are that it has been removed completely and that it does not show cancer.
Sessile polyps (sessile adenomas)
The term sessile is used to describe polyps that are slightly flattened and broad-based (as opposed to growing on a thin stalk).
Serrated polyps (serrated adenomas)
Serrated polyps (serrated adenomas) have a saw-tooth appearance when seen under a microscope. There are 2 types, which look a little different:
- Sessile serrated adenomas (also called sessile serrated polyps)
- Traditional serrated adenomas
These types of polyps are not cancer, but they are pre-cancerous (meaning that they can turn into cancer), so they need to be removed completely.
Someone who has had a serrated polyp has an increased risk of later developing colon or rectal cancer. However, most people with these polyps never develop colon or rectal cancer.
Dysplasia
Dysplasia describes how much your polyp looks like cancer under a microscope:
- Polyps that are only mildly abnormal (don’t look much like cancer) are said to have low-grade (mild or moderate) dysplasia.
- Polyps that are more abnormal and look more like cancer are said to have high-grade (severe) dysplasia.
If high-grade dysplasia is found in your polyp, it might mean you’ll need a repeat (follow-up) colonoscopy sooner than if it wasn’t found. But otherwise dysplasia in a polyp is not usually cause for concern.
The most important thing is that your polyp has been removed completely, and that it does not show cancer.
If an adenoma wasn’t removed completely…
If you had an adenoma that was biopsied but not removed completely, talk to your doctor about what other treatment you might need.
Most often, adenomas are removed during a colonoscopy. Sometimes, though, an adenoma might be too large to remove completely during the colonoscopy. If this is the case, you might need surgery to ensure that all of the adenoma is removed.
Does having an adenomatous polyp (adenoma) affect my follow-up care?
If an adenoma was found during your biopsy, you will need another colonoscopy at some point to make sure that you don’t have any more adenomas. When you should have your next colonoscopy depends on a number of things, like how many adenomas were found, if any had a villous growth pattern, and if any had high-grade dysplasia. Discuss the timing of your next colonoscopy with your doctor.
- Written by
The American Cancer Society medical and editorial content team
Our team is made up of doctors and oncology certified nurses with deep knowledge of cancer care as well as editors and translators with extensive experience in medical writing.
Last Revised: July 7, 2023
American Cancer Society medical information is copyrighted material. For reprint requests, please see our Content Usage Policy.
American Cancer Society Emails
Sign up to stay up-to-date with news, valuable information, and ways to get involved with the American Cancer Society.

