
Your gift is 100% tax deductible.
Your Breast Pathology Report: Atypical Hyperplasia (ADH or ALH)
Learn about some of the medical terms in a pathology report that shows atypical ductal hyperplasia (ADH) or atypical lobular hyperplasia (ALH).
Types of breast biopsies
A biopsy is a procedure that removes small pieces of tissue so they can be examined under a microscope or tested. A breast biopsy can be done by:
- Needle biopsy, where a hollow needle is used to remove samples from an abnormal area in your breast.
- Incisional biopsy, a type of surgical biopsy in which only part of an abnormal area is removed.
- Excisional biopsy, a type of surgical biopsy that removes the entire abnormal area, often with some of the surrounding normal tissue. It is much like a lumpectomy, a type of breast-conserving surgery.
After biopsy samples are collected from your breast, they are studied by a pathologist, a doctor who specializes in diagnosing and classifying disease. After testing the samples, the pathologist creates a pathology report on what was found. Your doctors can use this report to help manage your care.
What is hyperplasia?
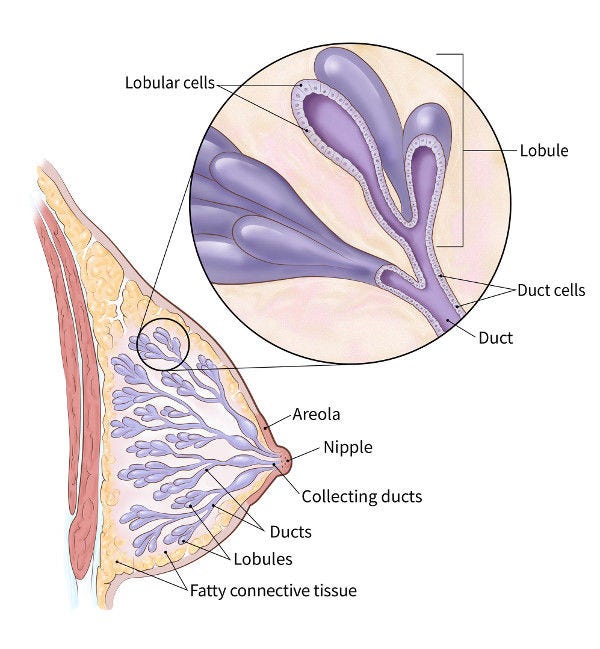
The normal breast contains milk ducts (tiny tubes) that end in groups of sacs called lobules (where milk is made). Normally, the ducts and lobules are lined by 2 layers of cells.
Hyperplasia means that there are more cells than usual within the ducts or lobules, and they are no longer lined up in just the 2 layers.
- Usual ductal hyperplasia (UDH), also called hyperplasia of the usual type or ductal hyperplasia without atypia, means the cell growth in the ducts looks much like the normal pattern under the microscope. It does not need to be treated, although it is linked to a slightly increased risk of getting breast cancer later on.
- Atypical hyperplasia, either atypical ductal hyperplasia (ADH) or atypical lobular hyperplasia (ALH), means the cell growth looks more abnormal.
Atypical ductal hyperplasia (ADH)
In ADH, cells in the ducts are growing in an abnormal pattern and have some but not all of the features of ductal carcinoma in situ (DCIS), which is a precancer. This means that ADH is not yet a precancer, although it is linked to an increased risk of getting breast cancer later on.
If ADH is found on a needle biopsy, more tissue in that area usually needs to be removed to be sure that nothing more serious is nearby, such as DCIS or invasive breast cancer. The tissue that is removed is looked at under a microscope, and if nothing more serious is found, no other treatment is needed.
If ADH is found on an excisional biopsy, usually no more surgery is needed, unless there’s concern that it might not have been removed completely.
Because having ADH increases your risk of breast cancer, your doctor might recommend:
- More frequent follow-up with breast exams and imaging tests such as mammograms
- Making lifestyle changes or taking medicine to help reduce your risk of breast cancer
Atypical lobular hyperplasia (ALH)
ALH is an abnormal growth of cells within lobules of the breast that is linked with an increased risk of breast cancer.
If ALH is found by a needle biopsy, doctors might advise:
- Close follow-up with physical exams and imaging tests, like mammograms.
- Removing more of the area around the biopsy site to make sure that there isn’t anything more serious nearby
If ALH is found by an excisional biopsy, typically no further treatment is needed.
Because having ALH increases your risk of breast cancer later on, your doctor might recommend:
- More frequent follow-up with breast exams and imaging tests such as mammograms
- Making lifestyle changes or taking medicine to help reduce your risk of breast cancer
Other benign breast changes
Other benign (noncancerous) changes that might be noted on a pathology report include:
- Adenosis
- Sclerosing adenosis
- Radial scar or complex sclerosing lesion
- Papilloma or papillomatosis
- Apocrine metaplasia
- Columnar cell change
- Collagenous spherulosis
- Duct ectasia
- Fibrocystic changes or cysts
- Flat epithelial atypia (FEA)
- Columnar alteration with prominent apical snouts and secretions (CAPSS)
These aren’t likely to be important if they’re seen on a biopsy sample that also contains ADH or ALH.
Microcalcifications or calcifications
Microcalcifications or calcifications are small calcium deposits that can be found in both noncancerous and cancerous breast lesions. They can be seen both on mammograms and under a microscope.
Because certain calcifications can be found in areas containing cancer, their presence on a mammogram might lead to a biopsy of the area. Once the biopsy is done, the pathologist looks at the tissue removed to be sure that it contains calcifications. If so, the doctor knows that the biopsy sampled the correct area (the abnormal area seen on the mammogram).
E-cadherin
Testing for E-cadherin might be done to help determine if hyperplasia is ductal or lobular. The cells in ADH are usually positive for E-cadherin, while the cells in ALH are usually negative for E-cadherin. If your report doesn’t mention E-cadherin, it means that this test wasn’t needed to figure out which type of hyperplasia you have.
Other lab tests
Other tests that are sometimes used to help diagnose different types of breast changes include:
- High molecular weight cytokeratin (HMWCK)
- CK903, also known as 34betaE12
- CK5/6
- p63
- Muscle specific actin
- Smooth muscle myosin heavy chain
- Calponin
Not all biopsy samples need these tests for an accurate diagnosis. If these tests appear on your pathology report, ask your doctor what the results mean for you.
- Written by
- References

Developed by the American Cancer Society medical and editorial content team with medical review and contribution by the American Society of Clinical Oncology (ASCO).
American Society of Breast Surgeons. Resource Guide: Surgical Management of Benign or High-Risk Lesions. 2024. Accessed at https://www.breastsurgeons.org/docs/statements/asbrs-high-risk-lesions.pdf on March 16, 2026.
Collins LC, Schnitt SJ. Chapter 9: Pathology of benign breast disorders. In: Harris JR, Lippman ME, Morrow M, Osborne CK, eds. Diseases of the Breast. 5th ed. Philadelphia, Pa: Lippincott Williams & Wilkins; 2014.
Hartmann LC, Degnim AC, Santen RJ, Dupont WD, Ghosh K. Atypical hyperplasia of the breast — Risk assessment and management options. N Engl J Med. 2015;372:78-89.
Orr B, Kelley JL. Benign breast diseases: Evaluation and management. Clin Obstet Gynecol. 2016;59(4):710-726.
Sabel MS. Overview of benign breast diseases. UpToDate. 2026. Accessed at https://www.uptodate.com/contents/overview-of-benign-breast-diseases on March 16, 2026.
Sabel MS, Collins LC. Atypia and lobular carcinoma in situ: High-risk lesions of the breast. UpToDate. 2026. Accessed at https://www.uptodate.com/contents/atypia-and-lobular-carcinoma-in-situ-high-risk-lesions-of-the-breast on March 18, 2026.
Last Revised: May 21, 2026
American Cancer Society medical information is copyrighted material. For reprint requests, please see our Content Usage Policy.
American Cancer Society Emails
Sign up to stay up-to-date with news, valuable information, and ways to get involved with the American Cancer Society.

