
Your gift is 100% tax deductible.
Prostate Cancer Research Highlights
The American Cancer Society helps men with prostate cancer in every community. And we’re funding research to help find more cures and save even more lives in the future.
What to Know About Black Men and Prostate Cancer
Studies show that Black men are 2 times more likely to die from prostate cancer than White men are. A main cause could be disparities in the accessibility and delivery of quality care.
Evidence keeps building that Black men are less likely to receive high-quality care for prostate cancer. When treatment is similar, prostate cancer 10-year survival is comparable or even higher among Black men.

Risk and Prevention Studies
Screening for Prostate Cancer Before and After COVID-19
Fewer men were getting screened for prostate cancer in 2023, after the COVID-19 pandemic, than they had been before it started in 2019. Read about the study.
Screening and Early Detection Studies
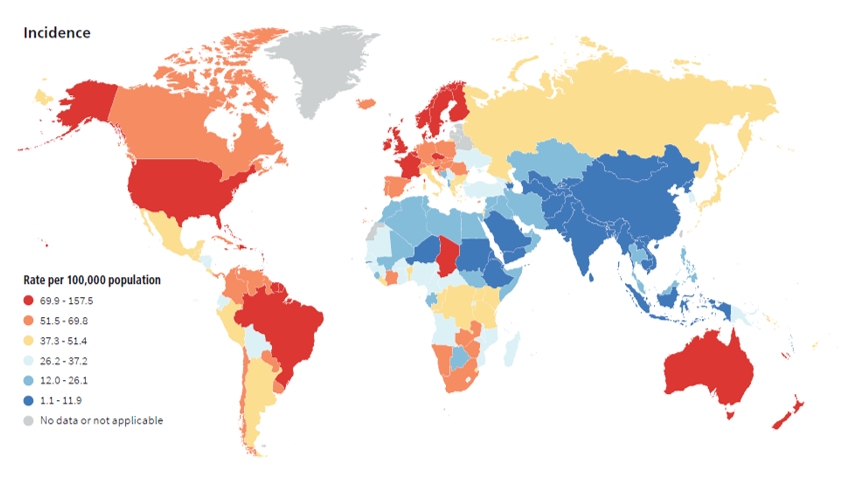
Prostate Cancer Incidence Rates Worldwide
Red countries: Have the highest incidence rates for prostate cancer, including the United States, Brazil, the Scandinavian countries, the British Isles, France, Australia, and New Zealand.
Dark blue countries: Have the lowest incidence of prostate cancer, including Niger, Sudan, and Ethiopia in Africa; Saudi Arabia; much of Central Asia; much of South Asia, including India; and much of East Asia, including Mongolia and China.
Treatment Studies
Eye-Opening Prostate Cancer Statistics
Survivorship Studies
More Prostate Cancer Research Stories
Prostate Cancer News
ACS Research Professors
ACS Statistics Reports
We Fund Cancer Researchers Across the US
The ACS funds scientists who conduct research about prostate cancer at medical schools, universities, research institutes, and hospitals throughout the United States. We use a rigorous and independent peer review process to select the most innovative research project proposals to fund.
Stats below are as of October 17, 2025.


