
Colorectal Cancer Drops in Older Adults and Rises in Younger Ones
The ACS 2026 Colorectal Cancer Statistics report says CRC incidence rates in the US are moving in two directions—down for 65+ and up for ages <65 (esp. in the distal colon and rectum).

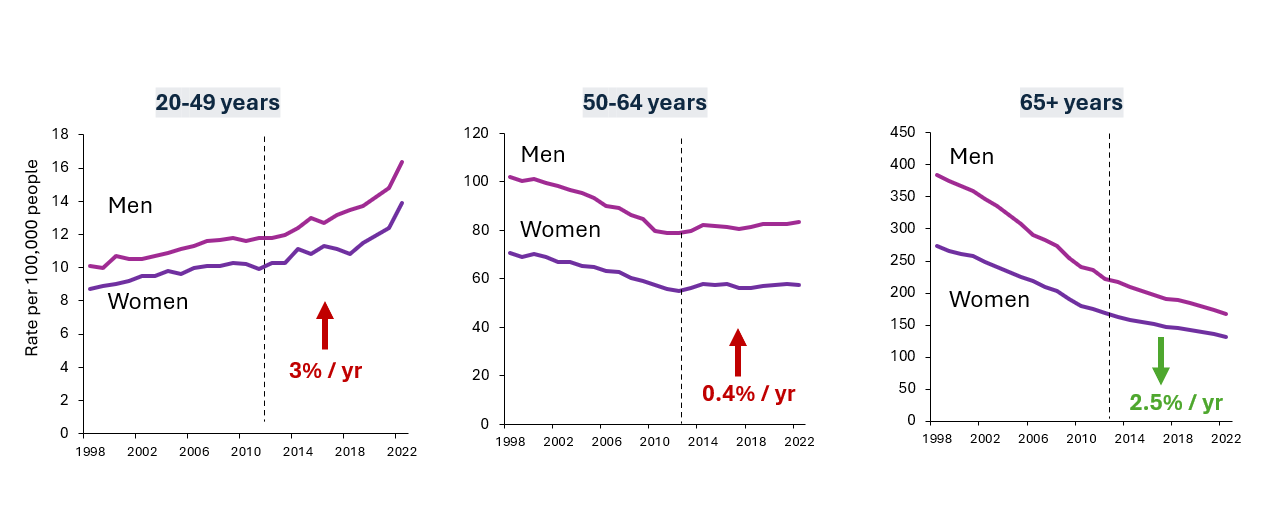
Colorectal Cancer Incidence Rates by Age and Sex, 1998-2022, United States
This graph shows incidence rates (vertical axis) by sex for three age-groups (20 to 49; 50 to 64; 65 and over) from 1998 to 2022 (horizontal axis). Incidence rates are increasing among younger men and women (<65) and decreasing among older adults (65+). Source: Colorectal Cancer Statistics 2026 Slideshow
In 2026, an estimated 158,850 new cases of colorectal cancer (CRC) will be diagnosed, and 55,230 people will die from the disease in the United States.
The Alaska Native population has the highest CRC incidence (81 cases per 100,000 people) and death rates (32 deaths per 100,000) in the world—more than twice that of White people in the United States. The American Indian population has the second-highest CRC burden in the US.
Here are more key facts from the "Colorectal Cancer Statistics report, 2026," published in the American Cancer Society (ACS) flagship journal CA: A Cancer Journal for Clinicians.
CRC is increasingly diagnosed in younger people (under age 65).
- As the graphic above shows, CRC incidence is rising in adults under 65 by 3% per year in people 20 to 49 and by 0.4% in those 50 to 64, while decreasing among those 65 and older by 2.5% per year. The increases are driven by cancer occurring in the sigmoid colon (the distal end of the colon closest to the rectum) and in the rectum.
- Early-onset CRC (diagnosis before age 50) incidence is rising for all racial-ethnic groups:
- Up 2% per year in Black people
- Up 3% per year in the Asian American and Native Hawaiian & Pacific Islander (AANHPI) population, American Indian and Alaska Native (AIAN) population, and the White population
- Up 4% per year in the Hispanic population
- In adults 65 and older, CRC both incidence and mortality have continued to decrease by more than 2% per year during the past 10 years.
It's clear that colorectal cancer can no longer be called an old person’s disease. We must double down on research to pinpoint what is driving this tsunami of cancer in generations born since 1950.”
Younger people (under 50) are getting diagnosed at advanced stages more often now than older adults (over 65).
- About 3 out of 4 adults younger than 50 with CRC are diagnosed when the disease is at an advanced stage, which can be either regional or distant stage. Within that group, 27% (about 1 out of 4) have distant stage CRC.
- Starting screening at age 45 works: Many CRC deaths can be prevented with more people getting screened because half of people diagnosed before 50 are ages 45 to 49 and that's the age range when people with an average risk are eligible for CRC screening. On-time screening can both prevent cancer by finding precancers that are easily removed and by finding cancer early, before symptoms develop, when they are usually more treatable. (See the prevalence of colorectal screening in your state.)
The incidence of rectal cancer is rising.
- Rectal cancer incidence increased in all ages combined by 1% per year from 2018 to 2022—after decades of decline.
- Of all CRC diagnoses, rectal cancer now accounts for about one-third (32%) of all cases, which is up from about one-fourth (27%) in the mid-2000s
Death rates for CRC are rising for people under 65.
- CRC is the most common cancer-related death in people under 50. (It’s the second most common cancer death overall.)
- In adults under 50, CRC death rates have increased by 1% per year since 2004, in contrast with declining trends for all other common cancers (breast, lung, prostate). For those ages 50 to 64, death rates have also increased 1% per year beginning 2019. In contrast, the death rate has dropped by 2 to 3% per year for people older than 65 since the 1990s.
There's an urgent need for research to discover the cause of rising CRC incidence in every generation born after the 1950s.
While researchers look for answers, several actions could help reduce the burden of CRC in the US, including:
- Earlier diagnosis through CRC screening. Clinicians, health centers, and states have the opportunity to increase the uptake of CRC screening starting at age 45 for those with an average risk of developing the disease. People who have a high risk, such as those who have a family history, may be advised to start screening at a younger age. (See the American Cancer Society CRC Screening Guideline.)
- Timely follow-up with colonoscopy for people who had a positive screening with a stool test.
- Educating the public about harmful lifestyle habits that may increase the risk of developing colorectal cancer:
- Drinking 3 or more alcoholic drinks a day
- Having a body mass index of 30 or greater
- Eating a lot of red meat and/or processed meat
- Having a diet low in fruits, vegetables, and other fiber
- Having low physical activity levels most days
- Smoking
- Educating the public about red flag symptoms of CRC: Rectal bleeding, abdominal pain, diarrhea, and iron-deficiency anemia to increase earlier detection and treatment.
- Educating clinicians about CRC symptoms and about paying greater attention to the unique needs of younger patients, including discussions about preserving fertility and sexual health
Incidence in the Colorectal Cancer Statistics, 2026 report is based on population-based cancer registries in the US, and mortality is from the National Center for Health Statistics.
The ACS researchers who coauthored this triennial report were Rebecca Siegel, MPH; Nikita Sandeep Wagle, MBBS, MHA, PhD; Jessica Star, MA, MPH; Tyler Kratzer, MPH; Robert Smith, PhD; and Ahmedin Jemal, DVM, PhD.
- Helpful resources
- For researchers
American Cancer Society news stories are copyrighted material and are not intended to be used as press releases. For reprint requests, please see our Content Usage Policy.

