
Your gift is 100% tax deductible.
Breast Reconstruction Using Your Own Tissue (Flap Procedures)
A tissue flap procedure uses tissue from your own body to rebuild the shape of your breast after cancer surgery. This is also called autologous or tissue-based reconstruction.
What is a tissue flap procedure?
These procedures use tissue from other parts of your body to rebuild your breast shape. The tissue might come from your belly, back, thighs, or buttocks.
In most cases, tissue flaps are used by themselves to rebuild the breast. Sometimes, an implant is also used if more fullness is needed.
These surgeries are usually more complex than implant surgery, and the recovery often takes longer.
Benefits and risks of tissue flaps
As with any surgery, it’s important to learn about the benefits and risks and talk them through with your healthcare team before you decide.
Possible benefits
The tissue from this type of surgery comes from your own body, so the new breast often looks and feels more natural than an implant.
Tissue flap reconstruction also acts more like a natural breast:
- It can get bigger or smaller if your weight changes.
- It does not need to be replaced over time like an implant.
- It may feel softer and more natural.
Possible risks or disadvantages
Tissue flap procedures are usually complex, and they involve more than one part of your body. Some possible concerns include:
- Longer surgery and recovery time
- The possibility that the flap may not survive, for some types of procedures
- Scars in two areas: the breast and the donor site where the tissue was taken
- Problems at the donor site, such as belly bulging, muscle weakness, or skin dimpling and other changes in shape
Many people heal well, but talk with your healthcare team about these risks and what to expect.
Can tissue flap restore feeling to the reconstructed breast?
Nerves are cut during a mastectomy. This causes a loss of feeling in that part of the chest. The skin on the chest wall can feel numb (no feeling) or it can be more sensitive. Feeling might return after a few months or years, or it might never return.
Finding ways to restore the feeling in the reconstructed breast has become a goal of tissue (flap) reconstruction.
It is often possible to keep a sensory nerve within the flap. A sensory nerve is a nerve that controls feeling. On the chest wall, a nerve in between the ribs is isolated and then reconnected with the nerve of the flap. This connection helps stimulate the tissue flap to regain feeling. Studies have shown improved sensation (feeling) using this technique.
Types of tissue flap procedures
Several types of flap procedures can be done for breast reconstruction. These are often named after the muscle or blood vessel used. For example: abdominal flap, back flap, or buttock flap.
Most fall into 2 main groups.
Pedicle flaps:
- Tissue is moved to the chest while staying attached to its original blood supply.
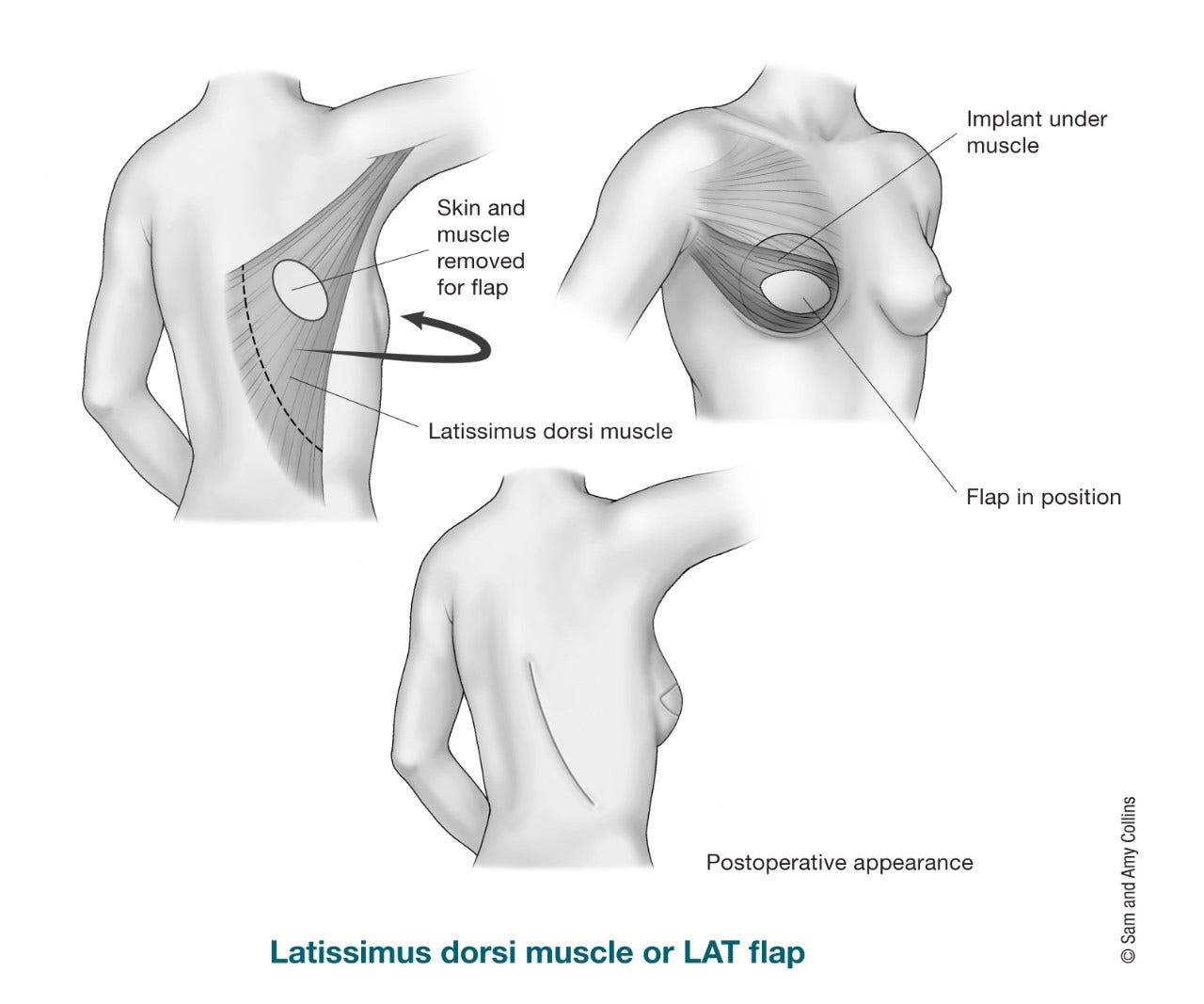
- The most common type is the latissimus dorsi (LD) flap, which uses tissue from the back.
- Tissue from the belly (TRAM flap) can also be used, but this is less common today.
Free flaps:
- Skin, fat, and sometimes a small amount of muscle is fully removed and moved to the chest. It does not stay attached to its original blood supply.
- Blood vessels are reconnected using microsurgery (a microscope). This makes the surgery take longer.
- Free flaps often preserve muscle. This may help keep strength and improve the look of the donor site.
- The belly is the most common donor site, but tissue can also come from the thighs, buttocks, or lower back.
- There is a small risk the flap may not survive if blood flow is not restored. You may need more surgeries if this happens.
Abdominal (belly) flaps
An abdominal flap uses tissue from your belly to rebuild your breast. There is often enough tissue to create the breast without needing an implant.
After this surgery, your belly may look like a “tummy tuck.” Depending on the type of flap, the surgery can affect your abdominal strength. It might also cause bulging. This option may not be suitable if you are very thin or have had a prior tummy tuck.
There are several types of abdominal flaps, depending on how the tissue is moved and how much muscle is used.
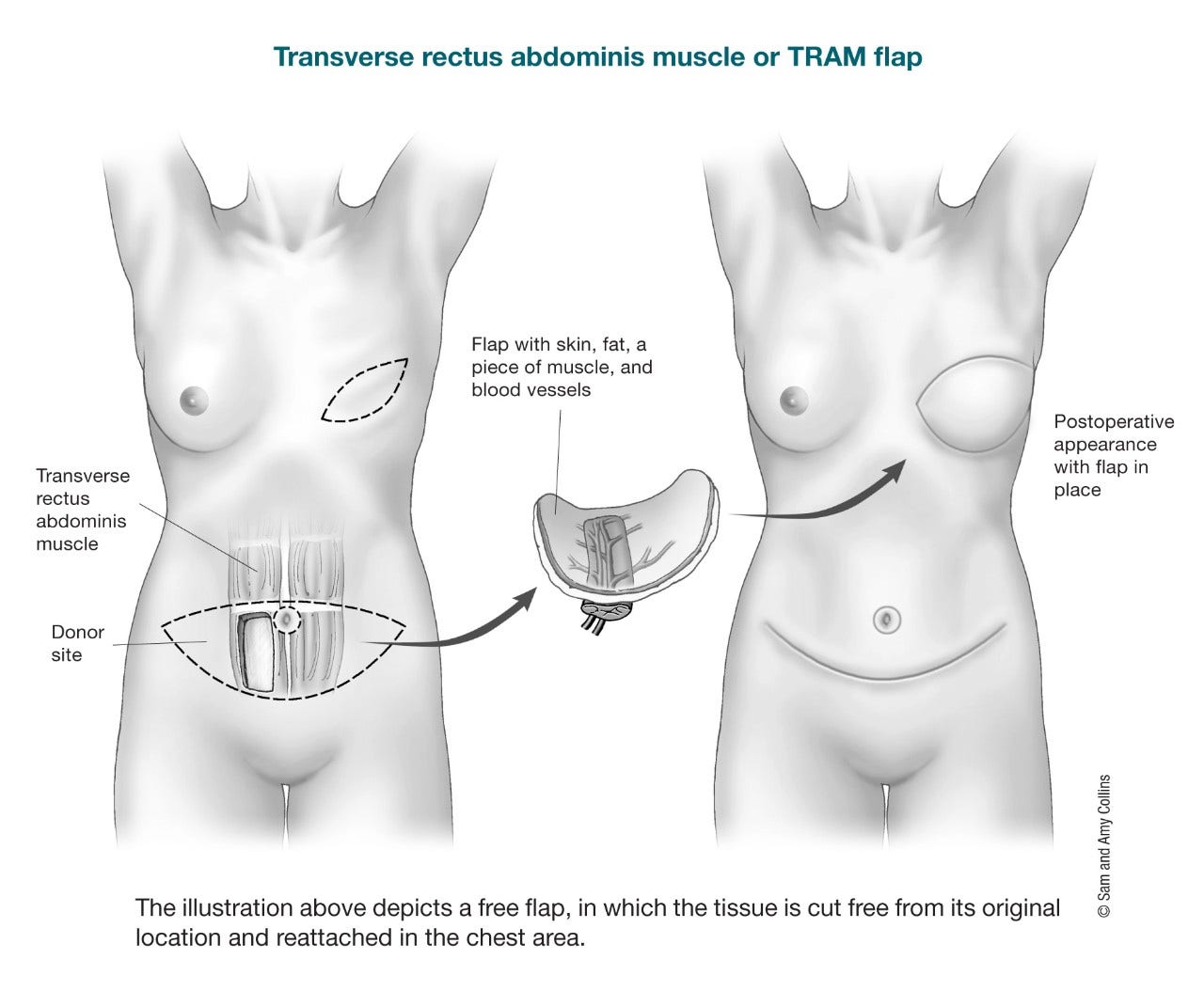
The TRAM (transverse rectus abdominis myocutaneous) flap uses skin, fat, and some or all of the rectus abdominis (six-pack) muscle. This can be done in 2 ways:
Pedicle TRAM flap:
- Tissue stays attached to its original blood supply and is tunneled under the skin to the chest
- Uses most or all of the rectus (six-pack) muscle on one side
- Higher risk of abdominal weakness or bulging
- Shorter surgery time than free flap options
Free TRAM flap:
- Skin, fat, and all or most of one rectus abdominis muscle is completely removed from the abdomen and transferred to the chest
- Blood vessels are reconnected using microsurgery
- Usually has better blood flow than pedicle TRAM
- Higher risk of abdominal weakness or bulging
- Small risk the flap may not survive if blood flow is not restored
These flaps also use tissue from the belly to rebuild the breast, but they are designed to better protect the abdominal muscle. Tissue is moved to the chest using microsurgery. The amount of muscle taken, if any, varies by type.
Muscle-sparing TRAM (MS-TRAM) flap
- Similar to a free TRAM, but only a small part of the muscle is removed
- Most of the abdominal muscle is preserved
- Lower risk of abdominal weakness and bulging
- Often gives a better appearance at the donor site (belly)
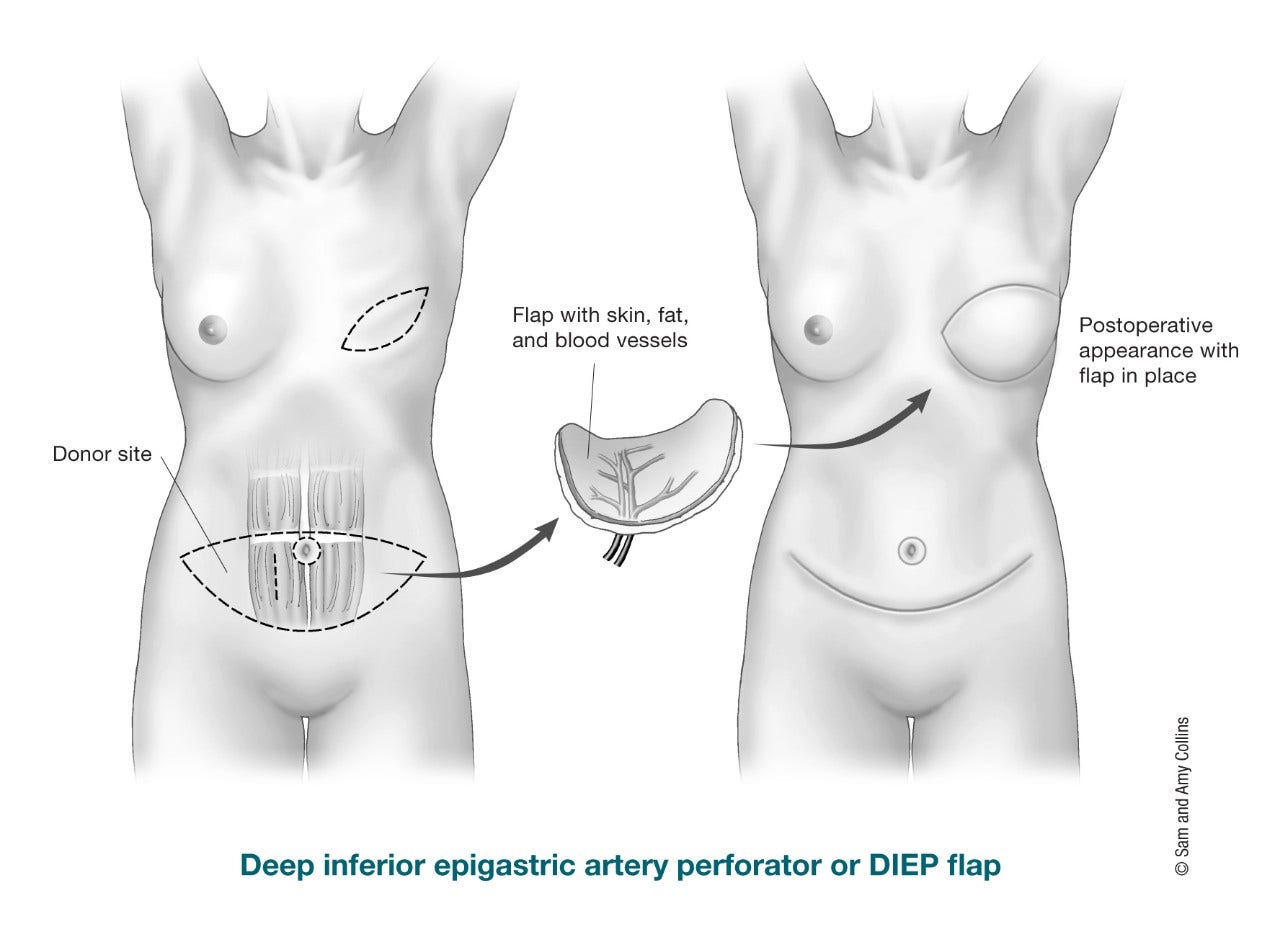
DIEP (deep inferior epigastric perforator) flap
- Uses skin and fat from the belly, similar to a TRAM flap
- Does not remove any abdominal muscle
- Tissue is fully removed and moved to the chest
- Blood vessels are reconnected using microsurgery
- Lower risk of abdominal weakness or bulging compared to TRAM flap
- Very similar to the muscle-sparing (MS-TRAM) flap, but no muscle is taken at all
SIEA (superficial inferior epigastric artery) flap
- Also uses skin and fat from the belly without taking muscle
- Uses blood vessels that are more superficial (closer to the skin) than the vessels used for DIEP flap
- Not everyone has these blood vessels, so fewer people are candidates
- Used less often than other abdominal flap procedures
Back flaps
A back flap uses tissue from your back to help rebuild your breast. This type of surgery is often considered when there is not enough abdominal (belly) tissue or when another type of reconstruction is not a good option.
- A pedicle flap that uses muscle, fat, and skin from the upper back
- Tissue is tunneled under the skin to the chest while staying attached to its blood supply
- Often combined with a breast implant or tissue expander to add volume
- May sometimes be used without an implant in select patients
- Most people do not notice major long-term weakness, though some may have mild changes in shoulder strength or endurance
- Uses skin and fat from the upper back but preserves the muscle
- Helps reduce the risk of muscle weakness compared to LD flap
- Often used for smaller reconstructions, such as after a lumpectomy or partial mastectomy
- May not provide enough volume for full breast reconstruction without additional procedures
- A newer free flap that uses skin and fat from the lower back (“love handle” area)
- No muscle is removed
- Blood vessels are reconnected using microsurgery
- Can provide moderate volume but is technically complex
- Usually done on one breast at a time and offered at specialized centers
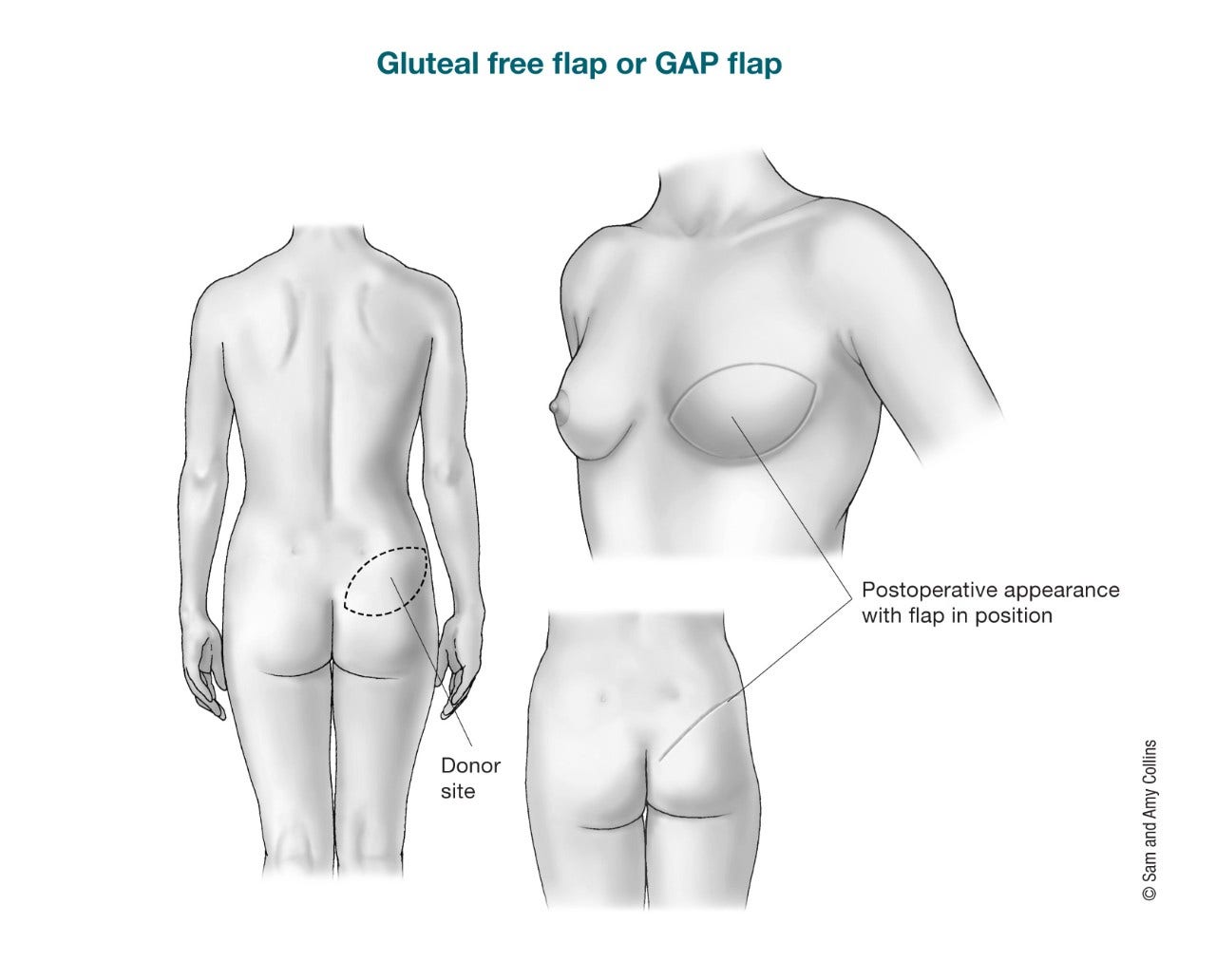
Buttock (bottom) flaps
Buttock flaps use tissue from your buttocks to rebuild your breast. This may be an option if you cannot or do not want to use tissue from your belly. For example, you might consider this type of surgery if you are thin or have had prior belly surgery.
- Uses skin and fat from the buttocks to form the breast
- Does not remove muscle
- Tissue is moved to the chest, and blood vessels are reconnected using microsurgery
This surgery might also be called:
- SGAP: uses tissue from the upper buttock
- IGAP: uses tissue from the lower buttock
It can be a good option if belly tissue is not available, but it is not offered at all hospitals. It may also cause dimpling or other changes to the shape of your buttocks. Sitting can be uncomfortable during recovery.
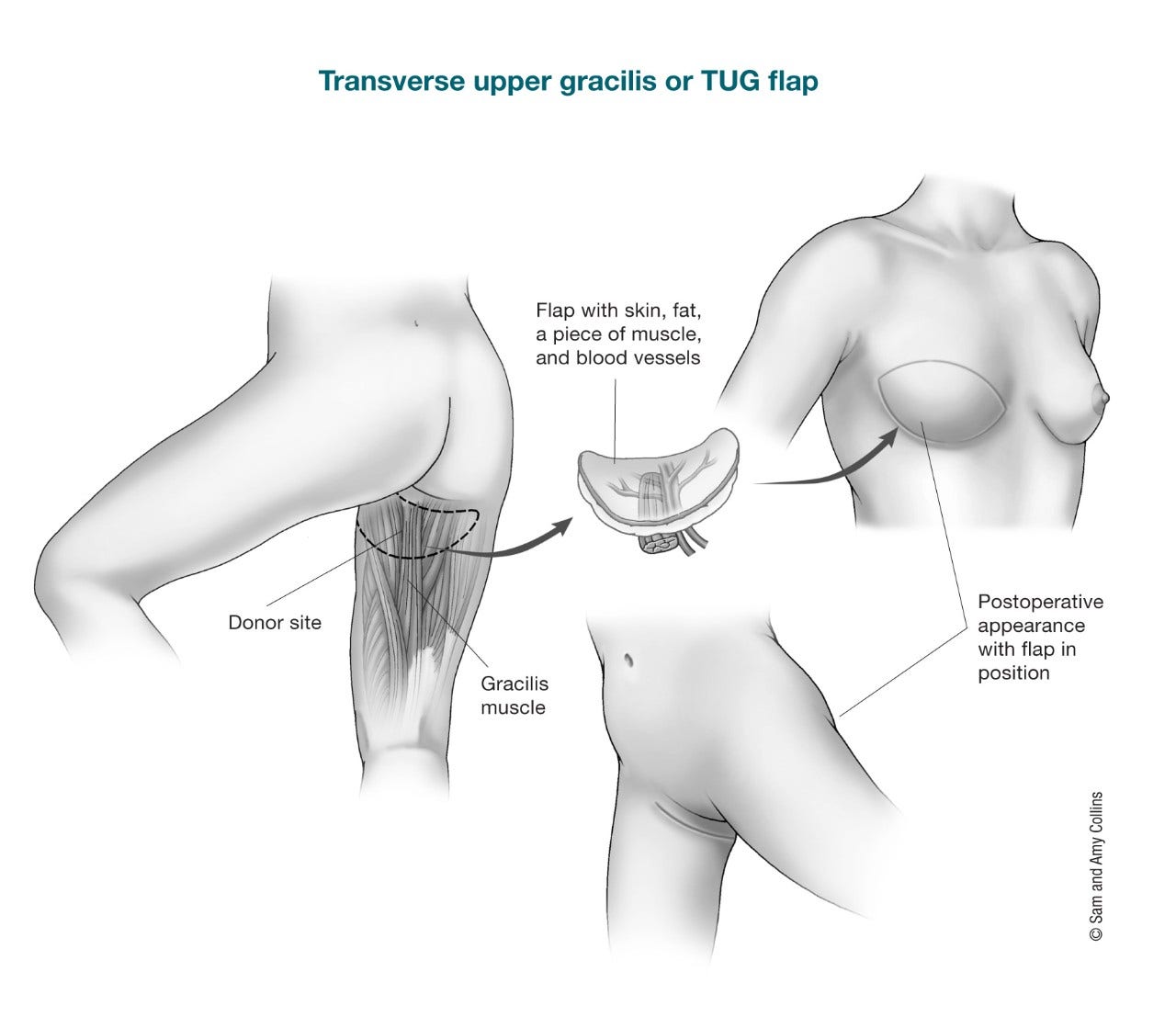
Thigh flaps
If tissue from your belly cannot be used, tissue from your thighs may be an option for breast reconstruction.
These procedures use microsurgery to move tissue to your chest and reconnect blood vessels. In most cases, the thighs provide enough tissue for a small to medium-sized breast. Sometimes, tissue from both thighs may be used to rebuild one breast.
- Gracilis flap uses skin, fat, and a small part of the gracilis muscle. These may be called TUG (transverse upper gracilis), VUG or VUP (vertical upper gracilis), or DUG (diagonal upper gracilis), based on the direction of the tissue.
- PAP (profunda artery perforator) flap uses skin and fat only, without removing muscle. It has become more common because it helps preserve muscle strength.
LTP (lateral thigh perforator) flap uses skin and fat from the outer upper thigh (“saddlebag” area) without removing muscle. It may be an option if abdominal tissue is not used.
- Written by
- References

Developed by the American Cancer Society medical and editorial content team with medical review and contribution by the American Society of Clinical Oncology (ASCO).
Abdou SA, Charipova K, Song DH. Modern Approaches to Pedicled Latissimus Dorsi Flap Breast Reconstruction with Immediate Fat Transfer. Clin Plast Surg. 2023 Apr;50(2):259-265.
American Society of Plastic Surgeons. Breast Reconstruction. Accessed at https://www.plasticsurgery.org/reconstructive-procedures/breast-reconstruction on March 10, 2026.
Beugels J, Bijkerk E, Lataster A, Heuts EM, van der Hulst RRWJ, Tuinder SMH. Nerve Coaptation Improves the Sensory Recovery of the Breast in DIEP Flap Breast Reconstruction. Plast Reconstr Surg. 2021;148(2):273-284. doi:10.1097/PRS.0000000000008160.
Beugels J, van Kuijk SMJ, Lataster A, van der Hulst RRWJ, Tuinder SMH. Sensory Recovery of the Breast following Innervated and Noninnervated Lateral Thigh Perforator Flap Breast Reconstruction. Plast Reconstr Surg. 2021;147(2):281-292. doi:10.1097/PRS.0000000000007547.
Escandón JM, Escandón L, Ahmed A, Weiss A, Nazerali R, Ciudad P, Langstein HN, Manrique OJ. Breast reconstruction using the Latissimus Dorsi Flap and Immediate Fat Transfer (LIFT): A systematic review and meta-analysis. J Plast Reconstr Aesthet Surg. 2022 Nov;75(11):4106-4116.
Jagsi R, King TA, Lehman C, Morrow M, Harris JR, Burstein HJ. Chapter 79: Malignant Tumors of the Breast. In: DeVita VT Jr, Lawrence TS, Rosenberg SA, eds. DeVita, Hellman, and Rosenberg’s Cancer: Principles and Practice of Oncology. 12th ed. Philadelphia, PA: Wolters Kluwer; 2023
Mehrara BJ, Ho AY. Breast Reconstruction. In: Harris JR, Lippman ME, Morrow M, Osborne CK, eds. Diseases of the Breast. 6th ed. Philadelphia, PA: Wolters Kluwer; 2022.
National Cancer Institute. Breast Reconstruction After Mastectomy. 2025. Accessed at https://www.cancer.gov/types/breast/reconstruction-fact-sheet on March 10, 2026.
National Comprehensive Cancer Network (NCCN). Practice Guidelines in Oncology: Breast Cancer. Version 2.2026. Accessed at https://www.nccn.org/professionals/physician_gls/pdf/breast.pdf March 9, 2026.
Thomsen JB, Rindom MB, Rancati A, Angrigiani C. Thoracodorsal artery flaps for breast reconstruction-the variants and its approach. Arch Plast Surg. 2021;48(1):15-25. doi:10.5999/aps.2020.01410.
Last Revised: July 1, 2026
American Cancer Society medical information is copyrighted material. For reprint requests, please see our Content Usage Policy.
American Cancer Society Emails
Sign up to stay up-to-date with news, valuable information, and ways to get involved with the American Cancer Society.

